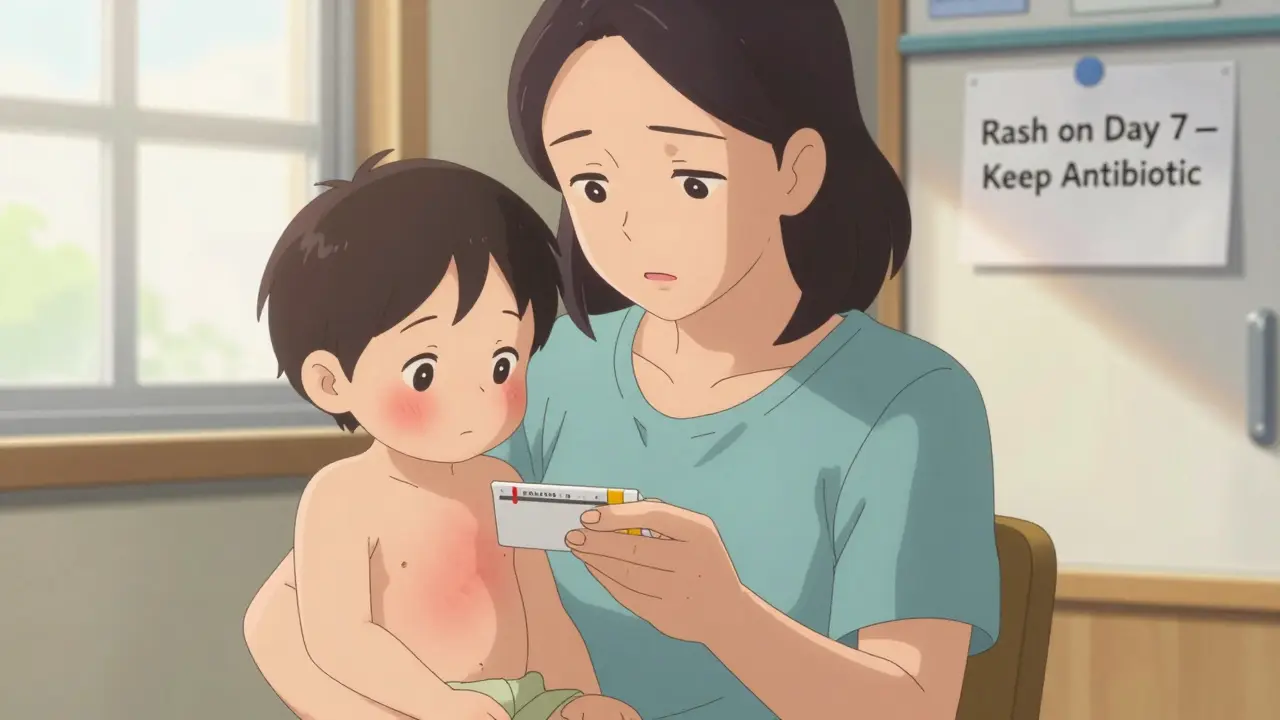
When your child breaks out in a rash after starting an antibiotic, panic is natural. You see red spots, feel the heat, and wonder: Is this an allergy? Should I stop the medicine? The truth is, most antibiotic rashes aren’t allergies at all-and stopping the drug could do more harm than good.
Most Rashes Aren’t Allergies
Over 90% of rashes that appear during antibiotic treatment-especially with amoxicillin-are not true allergic reactions. This isn’t a guess. It’s backed by data from Cincinnati Children’s Hospital and the CDC. A rash that shows up around day 5 to 10 of treatment, looks flat or slightly raised (maculopapular), doesn’t itch much, and stays in one place is almost always a harmless, non-allergic reaction. It’s not your body rejecting the drug. It’s often your body reacting to a virus, like Epstein-Barr, that you already have. Amoxicillin can trigger this kind of rash in 5 to 10% of kids, especially if they’re sick with a cold or flu. But the antibiotic? It’s still working.
True allergic reactions are rare. They happen fast-within an hour of taking the pill. The rash looks different: raised, red, itchy welts (hives) that move around your body. You might also get swelling in the lips or tongue, trouble breathing, or vomiting. These are signs of an IgE-mediated reaction, and they need immediate attention.
What to Look For: The Key Differences
Here’s how to tell them apart, simply:
- Non-allergic rash (most common): Appears 5-10 days after starting the antibiotic. Flat or bumpy red spots, mostly on the trunk, arms, or legs. Not itchy or only mildly itchy. Doesn’t spread quickly. No fever, no swelling, no trouble breathing.
- Allergic rash (rare): Comes on fast-within 1-2 hours. Raised, red, very itchy hives. Changes location. May come with swelling, coughing, wheezing, or nausea.
- Severe reaction (emergency): Rash with blisters, peeling skin, mouth sores, high fever (over 38.5°C), swollen lymph nodes, or flu-like symptoms. This could be Stevens-Johnson Syndrome or DRESS syndrome. Call 911 or go to the ER.
If you’re unsure, take a photo of the rash. Note the timing-when did the antibiotic start? When did the rash appear? Did your child have a cold or sore throat before the antibiotic? These details matter more than you think.
When to Keep Taking the Antibiotic
For the vast majority of rashes-non-itchy, no fever, no swelling-you should keep giving the antibiotic. Stopping it unnecessarily leads to bigger problems. Studies show that when parents stop antibiotics because of a rash, their child’s infection is 37% more likely to come back worse. They end up on stronger, broader-spectrum drugs like clindamycin or azithromycin. Those drugs increase the risk of severe diarrhea, including Clostridioides difficile, which can be life-threatening.
Doctors at Portland Pediatric and the CDC agree: if the rash looks non-allergic, continue the course. The rash will fade on its own in 5-7 days. You might even see it get a little worse before it clears. That’s normal. The antibiotic is doing its job.

When to Stop and Call the Doctor
Stop the antibiotic and call your doctor immediately if:
- The rash is accompanied by fever above 38.5°C
- There are blisters, peeling skin, or sores in the mouth, eyes, or genitals
- Your child has trouble breathing, swelling of the face or throat, or dizziness
- The rash spreads rapidly and looks like burns or raw skin
These signs point to serious conditions like Stevens-Johnson Syndrome or DRESS syndrome. These are rare-about 1 to 6 cases per million prescriptions-but they’re deadly if not treated fast. Don’t wait. Get help.
What to Do for Mild Itching
If the rash is non-allergic but a little itchy, you can ease discomfort without stopping the antibiotic. Use over-the-counter antihistamines like cetirizine (Zyrtec) or loratadine (Claritin). For kids, follow weight-based dosing: 0.25 mg per kg, up to 10 mg total, twice daily. You can also add famotidine (Pepcid), 0.5 mg per kg, up to 20 mg twice daily. Apply 1% hydrocortisone cream to itchy spots twice a day. Don’t use strong steroids. They won’t speed up healing and might hide signs of a deeper problem.
Why Mislabeling Rashes Is Dangerous
Here’s the scary part: if you label your child as “allergic to penicillin” based on a non-allergic rash, it can hurt their future health. The CDC reports that people with this mislabeling get different antibiotics 69% more often. Those alternatives are less effective, more expensive, and more likely to cause diarrhea, yeast infections, or drug-resistant bugs. In adults, mislabeled penicillin allergies are linked to a 30% higher risk of C. difficile infection and 30% higher death rates from sepsis.
And here’s the hopeful part: 92% of people who think they’re allergic to penicillin can safely take it again after proper testing. A simple skin test or oral challenge can clear the label. Many hospitals now offer these tests. Ask your doctor.
What Parents Are Saying
On parenting forums, stories flood in. One mom stopped amoxicillin after a rash. Her child’s ear infection returned worse. She had to switch to clindamycin-and then spent two weeks dealing with brutal diarrhea. Another parent, a pediatric nurse, says: “I’ve seen dozens of these rashes. When parents follow the doctor’s advice and keep going, 95% of kids heal fine.”
The pattern is clear: fear leads to stopping. Stopping leads to worse infections. Worse infections lead to stronger drugs. Stronger drugs lead to more side effects.
What Doctors Are Doing About It
Hospitals are catching on. In 2021, electronic health records started adding alerts like “Penicillin Allergy Reassessment.” By 2023, 87% of U.S. hospitals used them. These prompts remind doctors to question whether a rash was truly allergic. Kaiser Permanente cut down on incorrect allergy labels by 47% just by changing how they document rashes. Instead of writing “allergic to penicillin,” they now write: “Maculopapular rash on day 7 of amoxicillin-no systemic symptoms.”
New tools are coming. The FDA approved a 15-minute penicillin allergy test called PENtest in 2023. AI-powered smartphone apps are being tested to help parents identify rashes. One app, still in trials, correctly classified rashes 89% of the time.
Final Rule: Don’t Guess. Assess.
You don’t need to be a doctor to make the right call. Just ask:
- When did the rash start? (Before day 5? Likely allergic. After day 5? Likely not.)
- What does it look like? (Hives? Or flat red spots?)
- Is it itchy? (If yes, how bad? If no, it’s probably not allergic.)
- Is there fever, swelling, or trouble breathing? (If yes, go to the ER.)
If the answer is mostly “no” to danger signs, keep the antibiotic. Call your doctor to confirm. Don’t assume. Don’t panic. And don’t stop without asking.
Antibiotics save lives. A rash shouldn’t be the reason they’re stopped.
Can I give my child antihistamines for an antibiotic rash?
Yes, if the rash is non-allergic and itchy. Use cetirizine (Zyrtec) or loratadine (Claritin) at the child’s weight-based dose. You can also add famotidine (Pepcid) and apply 1% hydrocortisone cream to itchy areas. These help with discomfort but won’t make the rash go away faster. Do not use oral steroids unless directed by a doctor.
How long does an antibiotic rash last?
Non-allergic rashes usually appear 5-10 days after starting the antibiotic and fade within 5-7 days after stopping the drug-or even while continuing it. True allergic rashes (hives) can resolve in hours if the drug is stopped. Severe rashes like SJS or TEN take weeks to heal and require hospital care.
Should I stop amoxicillin if my child gets a rash?
Only if the rash is accompanied by fever, blisters, swelling, trouble breathing, or appears within 1-2 hours of taking the dose. If it’s a flat, non-itchy rash on day 6 or 7, keep giving it. Stopping it increases the chance of treatment failure and forces use of riskier antibiotics. Always call your doctor before stopping.
Can a child outgrow an antibiotic allergy?
Most children who develop a rash on amoxicillin aren’t truly allergic. Studies show that 92% of kids labeled as penicillin-allergic based on rash history test negative when evaluated. Even if a true allergy occurred once, many children outgrow it over time. A simple allergy test can confirm whether the allergy still exists.
Is there a test to confirm an antibiotic allergy?
Yes. For penicillin and related antibiotics, skin testing and oral challenges are safe and accurate. A new rapid test called PENtest gives results in 15 minutes. These tests are available at allergist offices and major hospitals. If you’ve been told your child is allergic based only on a rash, ask your doctor about testing-it could change their future treatment options.

Been there. Kid got a rash on day 7 of amoxicillin. No fever, no itching much. Kept going. Rash faded in 5 days. No drama. Doctors know what they're talking about.
Stop panicking. Trust the data.
The maculopapular eruption secondary to amoxicillin in the context of concurrent viral exanthem-particularly EBV-is a well-documented non-IgE-mediated phenomenon. The immunologic mechanism involves T-cell activation and cytokine dysregulation, not true hypersensitivity. Misclassification as penicillin allergy leads to suboptimal antibiotic stewardship and increased beta-lactam avoidance, which correlates with higher rates of MRSA and C. diff colonization.
Stop conflating benign exanthems with anaphylaxis. The data is unequivocal.
Why are we letting Big Pharma dictate what a rash looks like? They’ve been pushing this narrative for decades. You think they care about your kid? They care about selling more antibiotics and avoiding liability.
My cousin’s kid got a rash, kept the drug, ended up in the ICU with SJS. They didn’t even warn us.
Don’t be a sheep.
Wait-so you’re telling me the CDC and a bunch of hospitals are in on it? 87% of U.S. hospitals using alerts? That’s not a coincidence. That’s a controlled rollout.
Who funded the PENtest? Who owns the AI app? Pharma. They want you to keep taking antibiotics so you get hooked on their drugs. And now they’re rebranding rashes as ‘harmless’ to keep profits flowing.
Wake up. This is manipulation.
There’s a profound irony here: we are taught to fear the body’s natural response-rashes, fevers, inflammation-as if they are enemies to be suppressed, rather than signals to be interpreted.
Yet we simultaneously demand certainty, precision, and binary answers from complex biological systems.
Is this rash an allergy? The question itself is flawed. It presumes a single cause, when biology rarely operates in absolutes.
Perhaps what we need is not more algorithms or tests-but humility. To sit with uncertainty. To listen. To observe. To trust the process-not just the protocol.
Look, I get the science, I really do. But let’s be real-most parents aren’t reading CDC white papers. They’re scrolling at 2 a.m. with a feverish kid, heart pounding, wondering if they’re going to lose them. And then some guy in a lab coat says, ‘It’s fine, keep giving it.’
How is that not terrifying?
And don’t get me started on the fact that the moment you say ‘I think it’s an allergy,’ the doctor writes it down and it sticks for life. No one checks back. No one says, ‘Hey, let’s retest that.’
So yeah, maybe 92% of people aren’t allergic-but what about the 8% who are? And what about the ones who got misdiagnosed and then had to take clindamycin and got C. diff and spent six weeks in pain?
It’s not just about data. It’s about trauma. It’s about the fact that once you’re labeled, you’re stuck. And no one ever comes back to ask if you were wrong.
Let me tell you about my kid. She got the rash. I stopped the amoxicillin. We went to the ER. They said it was fine. We switched to azithromycin. She got diarrhea so bad she couldn’t walk. We had to go back. They said it was C. diff. We were in the hospital for five days. My wife cried for three nights.
Now I’m on every parenting forum screaming this: DON’T LISTEN TO THE DOCTORS WHO SAY KEEP IT GOING. THEY DON’T KNOW YOUR KID. THEY DON’T KNOW YOUR FAMILY. THEY JUST WANT TO CHECK THE BOX.
And then they write ‘penicillin allergy’ in the chart and you’re stuck with it for life.
They’re not saving your kid. They’re saving time. And your child is the cost.
As a pediatric nurse, I’ve seen this play out 40+ times. The rashes? Almost always benign. The panic? Always real. The outcomes? Way worse when parents stop the antibiotic.
It’s not about trusting doctors. It’s about trusting the pattern. Flat spots on day 7? No fever? No swelling? Keep going. The rash will fade. The infection won’t come back. And your kid won’t end up on a drug that wipes out their gut.
One mom said to me, ‘I didn’t know what to do.’ I told her: take a photo. Wait 24 hours. Call your doc. Don’t guess. Assess.
That’s all.